British health chiefs quietly sneak out warning that Pfizer and Moderna's vaccines may cause heart damage in 'extremely rare' cases
- Fears about link between the jabs and myocarditis have grown in recent weeks
- Now the UK's drug safety watchdog has updated safety information for the jabs
- It accepts that the condition is a possible side effect of both the Covid vaccines
British health chiefs quietly sneak out warning that Pfizer and Moderna's vaccines may cause heart damage in 'extremely rare' cases
- Fears about link between the jabs and myocarditis have grown in recent weeks
- Now the UK's drug safety watchdog has updated safety information for the jabs
- It accepts that the condition is a possible side effect of both the Covid vaccines
By Stephen Matthews Health Editor For Mailonline
Published: 13:08 EDT, 7 July 2021 | Updated: 14:33 EDT, 7 July 2021
British health chiefs have quietly released a warning that Pfizer and Moderna's Covid vaccines may cause heart damage, MailOnline can reveal.
Fears about the mRNA jabs' links to myocarditis have grown in recent weeks, following a string of cases in young adults and children in Israel and the US.
Now the UK's drug watchdog has updated its safety information to accept that the condition is a possible side effect of both vaccines, without a formal announcement.
The Medicines and Healthcare products Regulatory Agency insists the complication – inflammation of the heart muscle which can damage the organ over time – is still 'extremely rare' and 'typically mild'.
But it wasn't listed as a potential side effect until last week, when the MHRA released its most up-to-date safety surveillance data.
Cardiologists say the benefits of both jabs still clearly outweigh the risks for the vast majority of the population.
However, they say it 'completely changes' the debate about vaccinating children in Britain. They won't get AstraZeneca's jab because of its links to deadly blood clots in young people.
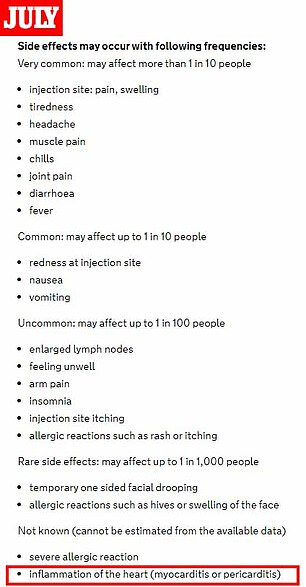

The UK's drug safety watchdog has updated its safety information to accept that myocarditis is a possible side effect of both vaccines (left). The MHRA insists the complication – inflammation of the heart muscle that can damage the organ over time – is 'extremely rare' and 'typically mild'. But it wasn't listed as a potential side effect until last week (pictured right, a screenshot of the same site last month), when the agency released its most up-to-date safety surveillance data.
Scientists had expected the protection given by vaccines to begin to wear off over time but they don't yet know how long immunity from jabs lasts for. Pictured, a stock image of jabs made by Pfizer and Moderna
MHRA statistics dated up until June 23 show 60 cases of myocarditis have been spotted among Pfizer vaccine recipients.
There have also been 42 cases of pericarditis – a similar condition that affects the protective layer around the heart.
Five instances of myocarditis and two of pericarditis have been detected in over-18s given Moderna's vaccines, the same figures show........