COVID-19 Vaccines: A “Cure” Worse Than the Disease?
The COVID-19 vaccines were released on an emergency basis before being properly tested. With the passage of time, the effects of these experimental drugs look increasingly dismal.
Lee D. Merritt MD
Many Americans have heard the news account of Dr. Gregory Michael, a 56-year-old Florida physician who, after receiving his first dose of the Pfizer/BioNTech COVID vaccine on December 18 of last year, was hospitalized with a blood disorder and spontaneous bleeding. In spite of being treated by a team of physicians, he died of a brain bleed due to total loss of his platelets — the little blood cells that stop bleeding. By February 10, 2021, 36 similar cases were reported in the mainstream media. Pfizer said in a statement that it was “aware of the death,” adding, “We are actively investigating this case, but we don’t believe at this time that there is any direct connection to the vaccine.”
Pfizer made this “finding” despite several unusual circumstances of the case. First, the low-platelet disorder known to most doctors as idiopathic thrombocytopenic purpura (ITP) most commonly affects children, and generally follows a viral illness. Only 10 percent of ITP cases occur in adults, who usually pre-sent with a slow onset form of the disorder, referred to as chronic ITP. The disorder usually starts by easy bleeding, such as slow oozing from gums or the nose, or bruises showing up without trauma. Rarely do platelets drop below 20,000 per microliter (normal levels are 200,000-500,000 per microliter), and generally treatment either reverses the disease or prolongs life for years in spite of the problem.
What happened to this physician and the others seems to be a new problem related to COVID vaccines, despite the manufacturers’ claims. This is further substantiated by the following case: After receiving the second dose of the Pfizer vaccine, a woman breast-fed her healthy one-month-old baby, who then died of thrombocytopenia.
Increasingly, vaccine manufacturers and government officials are following the sarcastic maxim from Samuel Shem’s novel of medical residency entitled The House of God: “If you don’t take a temperature you can’t find a fever.” In other words, if we don’t critically look at the actual recorded patient damage, we won’t find our products to be defective. Predictably, the major media — most of whose advertising money comes from Big Pharma — is increasingly getting on board, condemning “vaccine hesitancy” and pushing everyone to get vaccinated for COVID, discounting any dangers. But in the practice of medicine, we are supposed to employ the foundational principle of primum non nocere — first, do no harm.
Are These Really “Vaccines,” and Are They Necessary?
Moderna and Pfizer COVID-19 “vaccines” are experimental, employing a genetic technology never before used on humans. Ironically, many people who wouldn’t purchase the first edition of a new car model are lining up to take an injection they know nothing about, that has never successfully passed animal trials, that could never meet the required “safety level” for a “drug,” and that is unapproved for the prevention of COVID except as an emergency experiment. Legally, those who get the vaccine are unnamed participants in a Stage IV Food and Drug Admi-nistration (FDA) trial.
Moreover, a vaccine is supposed to prevent disease. By that definition, these agents are not vaccines. They are more properly termed “experimental unapproved genetic agents.” By admission of the manufacturers themselves, both the Pfizer and Moderna products only lessen the symptoms of COVID; they don’t prevent transmission.
Vaccination was first invented to treat smallpox, which had a fatality rate of up to 60 percent. Then other diseases such as typhoid and polio were similarly addressed. But vaccination should not be used when the death rate is low and effective, safe treatment is available. Although censorship has confused the public understanding, overwhelming evidence dating back to the 1970s shows that we have had success in treating viruses with lysosomotropic agents such as chloroquine. The current truth is that hundreds of papers have shown that chloroquine, and its later version hydroxychloroquine, is very effective in treating this virus if given early. A worldwide open architecture online review of COVID survival (hcqtrial.com) showed that the COVID death rate was 69.9-percent lower in those countries where hydroxychloroquine was used early and often.
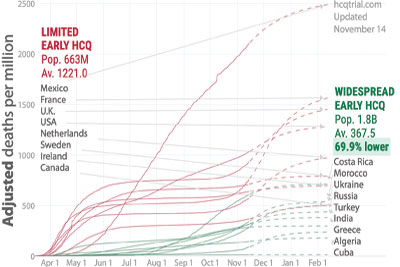
Safe and effective: As this graph shows, countries that used hydroxychloroquine widely to treat COVID-19 saw much lower death rates than those countries that restricted its use. (Photo credit: hcqtrial.com)
Multiple large studies done in outpatient settings show excellent results with hydroxychloroquine and other drugs such as ivermectin. In Mumbai, India, a study was done of the city police force of 10,000 officers. No deaths were recorded in the 4,600 officers taking a small dose of hydroxychloroquine each week. All the deaths were in the untreated group. Using Worldometer statistics, COVID deaths per capita in New York State are 2,770 per million population; in New Jersey they are 2,966 per million population. In India the rate is 273 per million, and in Uganda it is only 10 per million. Neither India nor Uganda used social distancing in any real way. But they do use hydroxychloroquine and ivermectin. New York (except for Dr. Zev Zelenko and a few others) has not used hydroxychloroquine. Recently, as the COVID death rate was increasing in India, the country defied WHO guidelines and started giving asymptomatic and mild COVID cases 200 mcg/kg of ivermectin daily for three to five days, and using both ivermectin and hydroxychloroquine for treatment. The disease and death rate immediately plummeted. Indian medical professionals cite 219 peer-reviewed studies proving the effectiveness of hydroxychloroquine, and 93 studies (54 peer-reviewed) that similarly show ivermectin’s benefit.
As to the claims of the efficacy of the experimental “vaccines,” the declaration of 95-percent effectiveness of the Pfizer product was shown to be false by Dr. Peter Doshi, the associate editor of the British Medical Journal. After doing an independent review of the data submitted to the FDA, Dr. Doshi reported that only about 19 percent of test subjects experienced the slightest benefit (symptom reduction). Absolute risk reduction — in other words, stopping transmission — he estimated at less than one percent. Interestingly, his excellent critique has been scrubbed from the Internet. (I have preserved a paper copy for any fact-checkers out there).
Every medical intervention is made after a risk-benefit analysis, i.e., do the potential risks outweigh the potential benefits? As seen above, the benefits have been highly overrated. During the first four months after the rollout of Pfizer and Moderna “vaccines” in 2021, 97 percent of deaths from vaccines recorded in the Vaccine Adverse Event Reporting System (VAERS) were for those agents, meaning only three percent of reported deaths involved all other vaccines combined. Here are the total deaths for all vaccines reported to VAERS, from January through April, during the years 2018-2021:
2018: 22 deaths
2019: 27 deaths
2020: 26 deaths
2021: 3,661 deaths
According to openvaers.com, as of this writing the VAERS database contains 5,888 reports of deaths following the COVID shots.
In Israel, where the Pfizer “vaccine” is being used exclusively and a major push is on to vaccinate the entire population, an independent review of government data after two months of the vaccine program was done by the Aix-Marseille University Faculty of Medicine Emerging Infectious and Tropical Diseases Unit’s Dr. Hervé Seligmann and engineer Haim Yativ. They showed that when 12.5 percent of Israelis were vaccinated, 51 percent of the deaths from COVID were in the vaccinated group. Additionally, in the over 65-year-olds, vaccination resulted in death from COVID 40 times more than in unvaccinated people. In other words, the Pfizer shot is not protecting people from COVID, but increasing fatalities from the disease — not to mention having other side effects.
If the truth were known, most sane, thinking people would not likely take part in such an experiment. With the truth suppressed, threats of travel bans, an unwarranted fear of COVID, and pressure from employers and the politicization of COVID in general, Americans have been throwing caution to the wind.
Bleeding and Thrombocytopenia
To understand what is actually happening to people after receiving the COVID “vaccines,” I reviewed bleeding and thrombocytopenia data in VAERS — an open-source searchable database of possible vaccine side effects reported by both providers and patients. According to the CDC website:
VAERS is used to detect possible safety problems — called “signals” — that may be related to vaccination. If a vaccine safety signal is identified through VAERS, scientists may conduct further studies to find out if the signal represents an actual risk.
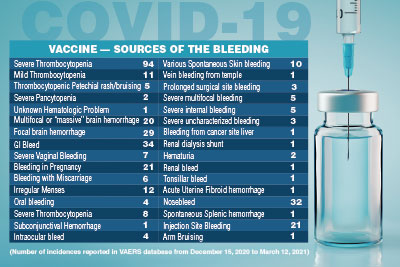
image:ffikretow/GettyImagesPlus
The main goals of VAERS are to:
• Detect new, unusual, or rare adverse events that happen after vaccination
• Monitor increases in known side effects, like arm soreness where a shot was given
• Identify potential patient risk factors for particular types of health problems related to vaccines
• Assess the safety of newly licensed vaccines
• Watch for unexpected or unusual patterns in adverse event reports
• Serve as a monitoring system in public health emergencies
The CDC acknowledges limitations of the system, including:
• Reports submitted to VAERS often lack details and sometimes contain errors.
• Serious adverse events are more likely to be reported than mild side effects.
• It is generally not possible to find out from VAERS data if a vaccine caused the adverse event.
I searched the VAERS database using keywords that would identify bleeding problems and thrombocytopenia (low or absent platelets). Entries are defined by age groups and sex with a narrative account of the injury. Keep in mind that these reports can be submitted by patients, caregivers, family members, and nurses. Doctors rarely report for a variety of reasons, including unfamiliarity of the system and time constraints. Insufficient details in the narrative are not correctable, nor does any one report conclude causality. The idea is to amass enough data points to recognize a trend.
In the two-and-a-half-month period from December 15, 2020 to March 12, 2021, 358 cases of unusual clotting or bleeding were identified, and it makes grim reading. There were 104 cases of frank thrombocytopenia (low platelets) — some including young people. However, the numbers alone do not adequately convey the problems. A physician documented this case of a young woman, aged 18-29: “Patient was seen in my office on 1/19/21 with complaint of heavy vaginal bleeding. A CBC was obtained which revealed an H/H of 12.2/36.1 and a platelet count of 1 (not 1K, but 1 platelet!) This was confirmed on smear review.” The surprise and horror the doctor experienced upon seeing the absence of platelets is clear when reading the report.
But the platelet problem may just be the most severe expression of a physical derangement that is producing bleeding of all sorts. As seen in the table on page 13, there were 49 people with brain hemorrhages — nine fatal at the time of reporting. A number of other people arrived at emergency departments with bleeding from multiple sites, or internally, so massive that they could not be stabilized even to clearly define the sources of the bleeding.
Most cases of severe bleeding were in people over age 50, but there were many younger people involved, especially in the less-severe-but-unusual bleeding problems. Of the 32 reported nosebleeds, six were either unable to be stopped with usual measures, were recurrent, or were recorded as leading to significant blood loss or dubbed “profuse.” Many bleeding issues were associated with other symptoms, such as photophobia (eye sensitivity to light), headache, hives, “sick in bed,” brain fog, and face swelling. The youngest patient with a nosebleed was, sadly, a toddler requiring emergency care. Unusual skin bleeding was also reported. Four 65-plus-year-old males reported blood spontaneously oozing through the skin: one from the legs, one from the scalp, one from an old biopsy site, and one from an old healed “boil” site. Frank bleeding at the time of inoculation occurred 14 times. Some bleeding was momentary, but often the bleeding was difficult to stop, was recurrent, and/or persisted after the patient returned home. Perhaps the saddest were the bleeding episodes that preceded spontaneous miscarriages.
Here are some direct entries in VAERS:
• 40-49 y.o. Female: The evening of my vaccination I began to feel feverish, weak and achy. During the night I woke with heavy bleeding and found out the following morning I had miscarried my otherwise healthy pregnancy.
• 39 y.o. Female: Internal brain bleeding 10 days after 1st dose Covid vaccine; brain damage, confused, suffering memory loss; This is a spontaneous report from a contactable physician (patient).
• 30-39 y.o. Female: 48 hours after injection developed micro-hemorrhages in her right eye. Symptoms resolved and 12/29 recurrence of bleeding to right eye slightly worse than before.
• 65+ y.o. Male: Patient developed significant nose bleed after receiving vaccine. Required emergency department visits x 2 and hospitalization.
• 65+ y.o. Female: Vaccine administered 02/02/2021. By Thursday 2/11/2021 patient almost nonverbal, by Monday 2/15/2021 patient went to the hospital with bruising, sores on her stomach and clots reported as thrombocytopenia. Deceased by Friday, 2/19/2021.
• 40-49 y.o. Female: Bleeding, myalgia, tingling in the fingers of the right hand; fatigue immediately upon vaccination — bleeding at the injection site which the employee reports as filling the Band-Aid over the site. When she got home in the evening and took it off blood ran.
• 65+ y.o. Female: Within 15 min of the injection, the individual became aphasic and stroke like symptoms. She was taken to the ER where she was later diagnosed with a cerebral hemorrhage and passed away.
When such facts are presented, the standard retort from vaccine advocates is, “We have given millions of vaccines, so a few deaths are to be expected.” Besides the fact that a willingness to sacrifice individuals for the nebulous good of the masses represents a bankrupt moral order, simply calculating the numbers of deaths is inadequate. Experts need to take the time to read the narrative to open their eyes — and their hearts — to the suffering happening. There are over 25 pages of such stories printed from VAERS entries, and we must ask, how many of these people are now dead, and how many are going to die?
Just before this article went to press, I attempted to update the numbers of the study. Now, using the same search terms and methodology, for the same time period of vaccination, instead of 358 reports there were over 6,200 reports. With any new medical intervention or drug rollout, this lag in reporting side effects produces an “avalanche effect” — a problem begins slowly and is barely perceptible, then speeds up unnoticed until it is too late to avoid the calamity. Looking at this data set, another finding was the greatly expanded degree of detail in the newer reports. This clearly reflects an awakened concern by medical professionals and others as to the seriousness of what they are witnessing.
A second-year medical student armed with the facts should recognize the ongoing disaster — where are the experts?
The “Unknowns” Outnumber the “Knowns”
In truth, neither COVID “vaccine” recipients nor their doctors know what is in these shots. Only a few people at the top of the Moderna, Pfizer, Johnson & Johnson, and AstraZeneca research groups really understand them. These injections produce a potentially deadly pathogen — a spike protein — in your cells.
COVID-19 Vaccines: A “Cure” Worse Than the Disease? - The New American